
key takeaway
California’s Behavioral Health Services Act (formerly MHSA) now directs more funding toward behavioral health care, housing, and treatment for people experiencing or at risk of homelessness. As counties prepare to implement new integrated plans by 2026, the BHSA will play a critical role in shaping partnerships across the behavioral health and housing continuum.
California’s county-provided behavioral health services, which address mental health conditions and substance use disorders, are essential to ensuring all Californians have access to care regardless of their race, age, gender identity, sexual orientation, or the county they call home. However, funding to support individuals with behavioral health conditions who are also facing housing instability or homelessness has been scarce.
The MHSA was initially passed in 2004 and established a millionaire’s tax to increase funding for mental health services, with 90% of the revenue allocated directly to counties. These services are typically administered by county behavioral health departments, though in rare cases other local entities, such as cities, provide them instead. (For the purposes of this report, “counties” refers collectively to counties, county behavioral health departments, and other local entities that administer MHSA/BHSA funds.)
The reforms under Prop. 1 aim to provide more targeted funding for behavioral health services and for housing or treatment units serving people with these conditions who are experiencing or at risk of homelessness. These funds are vital to California’s behavioral health system, accounting for nearly one-third of all county behavioral health services funding, and are now viewed as a critical piece in solving homelessness.
Prop. 1 renamed the Mental Health Services Act to the Behavioral Health Services Act (BSHA) and made other key reforms, including:
- Restructuring how existing funds are allocated, with a new stand-alone category for housing interventions.
- Expanding its scope to encompass treatment for substance use disorders.
- Changing the requirements for counties’ three-year program and expenditure plan for behavioral health services and outcomes.
- Revising accountability and transparency requirements for counties.
Prop. 1 also created a $6.38 billion general obligation bond to fund behavioral health treatment beds, residential facilities, and supportive housing for veterans and people at risk of or experiencing homelessness with behavioral health challenges. These funds are administered through Homekey+ and the Behavioral Health Continuum Infrastructure Program.
With counties set to begin implementing their BHSA Integrated Plans by July 1, 2026, this FAQ covers key timelines, opportunities for collaboration, and essential points that affordable housing developers, homeless service providers, and county staff should be aware of to strengthen partnerships within the behavioral health and housing continuum.
jump to:
- How is the Behavioral Health Services Act (BHSA) funding different from the Mental Health Services Act (MHSA)?
- What is a County Integrated Plan?
- What types of housing and housing supports can BHSA be used for?
- Who is eligible to benefit from BHSA housing funds?
- What government entities are in charge of disbursing BHSA funding?
- How and when are counties planning on disbursing BHSA funding?
- How can housing developers and homelessness service providers participate in BHSA planning?
- How can housing developers or service providers access BHSA funding for services, operating costs, or capital development funding?
- How much will my county receive in BHSA funds?
- How does BHSA intersect with other funding sources, like Transitional Rent?

About This Report
This publication was done in collaboration with Housing California.
Housing California brings together a diverse, multi-sector network to prevent and end homelessness, increase the supply of safe, stable, affordable housing options, and reverse the legacy of racial and economic injustice by building power among the people most impacted by housing injustice, shaping the narrative, and advocating for statewide policy solutions.
How is the Behavioral Health Services Act (BHSA) funding different from the Mental Health Services Act (MHSA)?
Under BHSA, counties continue to receive 90% of the funding, however, the spending categories will change beginning in 2026. Most counties will now have to allocate their BHSA funds as follows:
- 30% for housing interventions
- 35% for Full Service Partnerships
- 35% for behavioral health services and supports
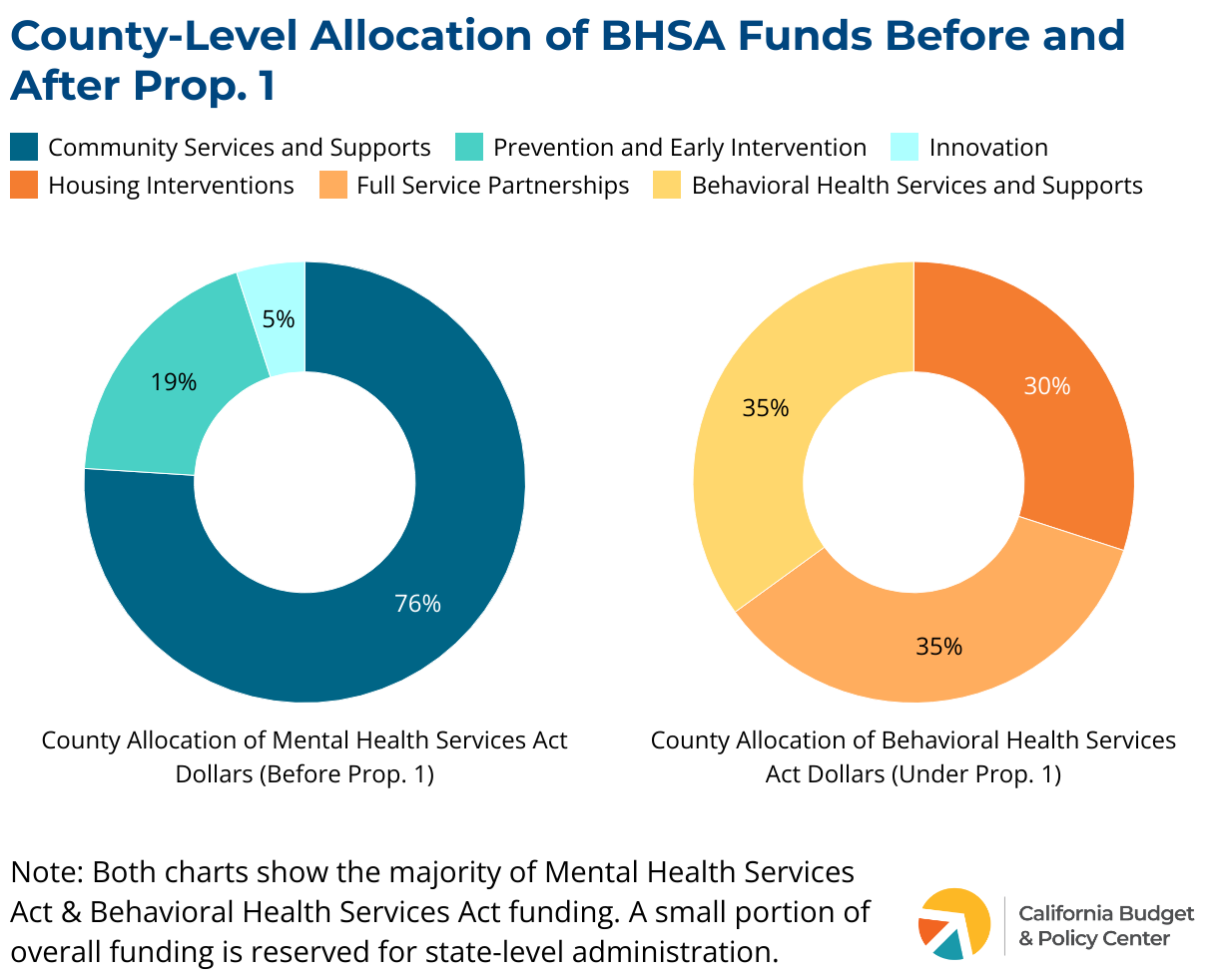
The restructuring of funds means counties are cutting back on vital services, especially in prevention and early intervention, innovative behavioral health programs, and other core services that primarily support children and youth. At the same time, counties are exploring ways to count existing efforts under the housing interventions category, since many have already used MHSA funds to provide housing or housing supports to individuals with behavioral health conditions.
Counties will have the flexibility to move up to 7% between BHSA categories to better meet local needs, which means housing intervention dollars may vary by county. Some could apply to move an additional 7% from the remaining category, for up to a 14% increase to housing interventions. However, small counties with populations under 200,000 can request exemptions from certain housing funding requirements starting with the 2026–29 Integrated Plan (IP). All counties, regardless of size, may request exemptions beginning with the 2032–35 Integrated Plan. Within housing, exemptions could apply to the 30% housing set-aside, the 50% requirement for people experiencing chronic homelessness, or the 25% limit on capital projects.
Reporting
Prop. 1 also changes the way counties plan and report behavioral health funding. Counties will now report on all behavioral health funding through their Integrated Plans, not just BHSA dollars. This includes local, state, and federal funding sources such as opioid settlement funds, SAMHSA and PATH grants, realignment funding, and federal financial participation.
What is a County Integrated Plan?
The BHSA establishes county Integrated Plans (IPs) to serve as a three-year prospective spending plan that describes how county behavioral health departments plan to use all available behavioral health funding, including BHSA. The first IP will span FY 2026-2029. It requires a robust community planning process and approval from the county board of supervisors. Counties are required to provide annual updates, which do not require stakeholder engagement. For more information, see How and when are counties planning on disbursing BHSA funding?
What types of housing and housing supports can BHSA be used for?
BHSA requires that 30% of the dollars a county behavioral health department receives be used on housing and housing-related supports, unless an exemption is approved. For FY 2026-27, DHCS projects the total annual statewide housing component will be approximately $950 million to be distributed among all counties.
The housing interventions offered must follow Housing First approaches in both interim and permanent housing settings, as defined by the Housing First statute, which is geared toward providing low-barrier, harm-reduction focused support. The expanded scope of housing interventions are intended to cover a range of needs and supports.
Critically, counties must first utilize housing-related services funded through Medi-Cal managed care plans (MCPs) before using BHSA funds for housing services. BHSA funds can only cover Community Supports if the MCP has declined to provide the service, the individual is ineligible, or the individual’s needs exceed MCP service limits. For more information see How does BHSA intersect with other funding sources, like Transitional Rent?.
Who is eligible to benefit from BHSA housing funds?
BHSA dollars can now be used to fund services, assistance, and housing for people who are at risk of or experiencing homelessness and have a serious mental health condition or substance use disorder. At least 50% of the housing intervention funds must serve people experiencing chronic homelessness.
County behavioral health departments deliver services directly or partner with housing developers, service providers, and other community organizations to carry out services. Within this population, counties can prioritize different subpopulations, so who BHSA interventions serve can look different by region.
What government entities are in charge of disbursing BHSA funding?
The state passes the revenues collected for BHSA directly to counties. Counties then task their behavioral health departments with the responsibility of disbursing or contracting BHSA funds.
How and when are counties planning on disbursing BHSA funding?
BHSA fund allocations are ultimately determined by each county’s Integrated Plan (IP), which covers a three-year period. IPs are intended to outline all county behavioral health activities, services, and funding streams, including BHSA, Medi-Cal, and other sources. It describes the activities and expenditures a county plans to fund with BHSA, ultimately providing a roadmap for the funds.
What an IP funds can vary widely depending on county size, location, local revenue streams, and community needs. Counties must also distribute funding in accordance with the new categorical percentages outlined in the BHSA, though some flexibility is allowed (see How does BHSA differ from MHSA?).
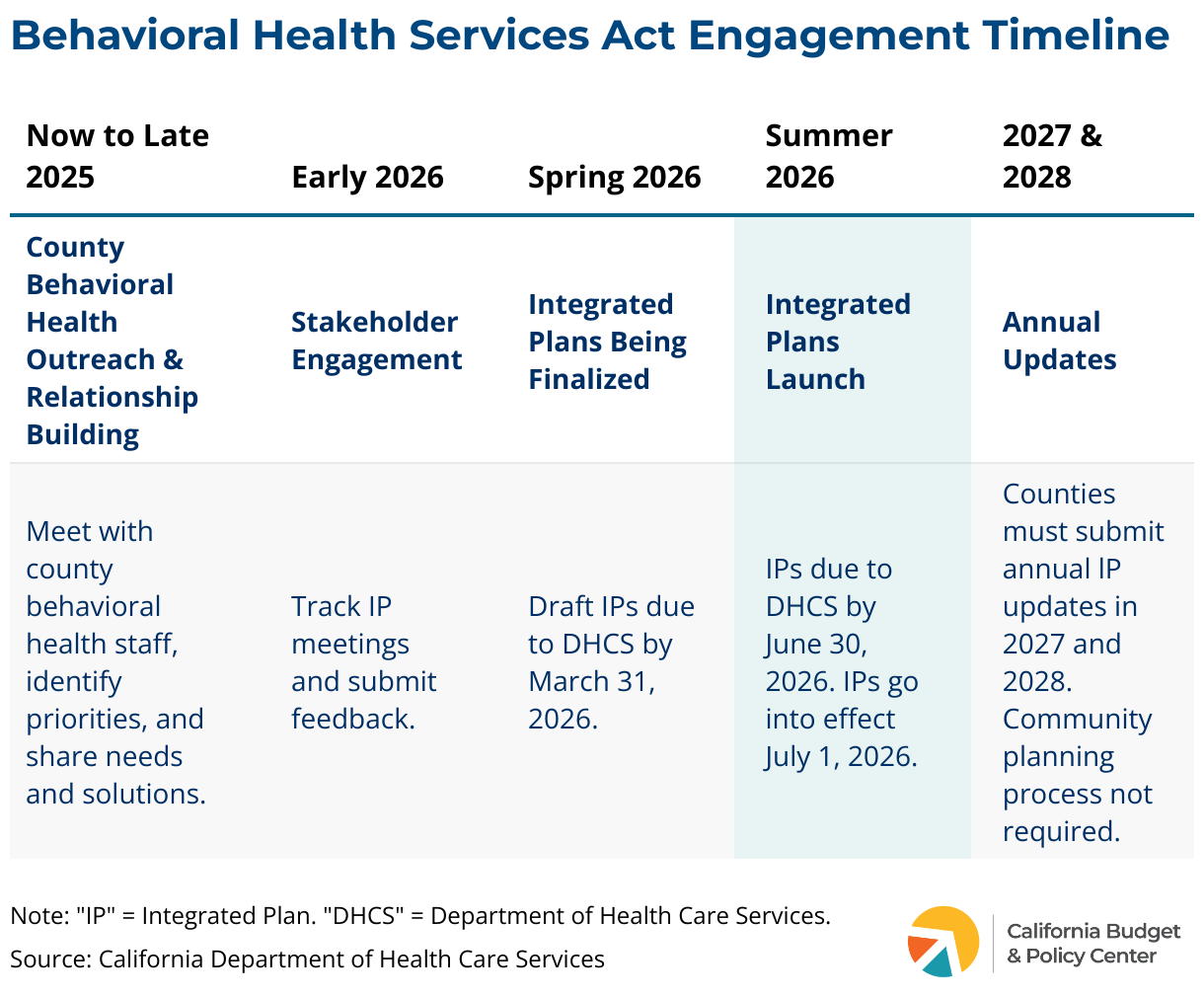
The first IP under the new BHSA guidelines will span FY 2026–2029. Counties are required to submit their initial draft IPs to the Department of Health Care Services by March 31, 2026, get approval from their Board of County Supervisors, and begin implementing it on July 1, 2026.
There is a community planning process which counties must go through, which is where housing developers and service providers can get involved. For more information on how to get involved, see How can housing developers and homelessness providers participate in BHSA planning?.
Separate funding from the bond portions of Prop.1 through the Behavioral Health Continuum Infrastructure Program (BHCIP) and Homekey+ have already begun to be awarded by the Department of Housing and Community Development.
How can housing developers and homelessness service providers participate in BHSA planning?
Counties must submit their initial draft of their 2026-2029 Integrated Plan (IP) to the Department of Health Care Services (DHCS) by March 31, 2026, which requires a community planning process. If a type of program, service, or strategy isn’t in the IP, it likely won’t receive BHSA support unless the plan is amended. Counties are currently holding integrated planning discussions and beginning their community planning process, during which they must coordinate with various stakeholders such as Continuums of Care, Medi-Cal Managed Care Plans, and providers of mental health services. Counties are not mandated to reach out to housing providers as a part of this Integrated Planning process, which is why proactive outreach is critical.
Now is the time for housing developers and homelessness service providers to start meeting with county behavioral health staff to:
- Build relationships and identify potential areas of collaboration
- Clarify which populations the county intends to prioritize, ensuring prioritization of high-need populations
- Spot possible project overlap and opportunities for joint efforts
- Explore ways to strengthen coordination and referrals between the county behavioral health system and the Continuum of Care
- Identify how BHSA dollars could help address current funding gaps, challenges, or scale innovative housing solutions
The county board of supervisors must approve the final IP by June 30, 2026, but before that, each plan must go through a 30-day public comment period. IPs take effect July 1, 2026.
As part of the required community planning process, counties must engage designated local stakeholders in developing the IP. This explicitly includes Continuums of Care, homeless service providers, mental health and substance use disorder treatment providers, county social services and child welfare agencies, and health care service plans, including Medi-Cal Managed Care Plans (MCPs). Counties with populations greater than 200,000 must also engage with the five most populous cities in their jurisdiction which is another point of collaboration for developers and service providers.
After the IP is approved in 2026, counties must submit annual updates in 2027 and 2028. These updates do not require a formal community planning process, which is why maintaining strong, ongoing relationships with county behavioral health departments and other key partners is essential.
Now is a key opportunity for affordable housing developers, homeless service providers, and housing advocates to be proactive. Their input is critical for helping counties identify barriers, such as insufficient housing stock, high development costs, or service delivery challenges, and for ensuring Integrated Plans include collaborative, actionable strategies to reduce homelessness and expand permanent housing options for people with behavioral health needs.
How can housing developers or service providers access BHSA funding for services, operating costs, or capital development funding?
BHSA dollars will flow through counties, which then decide how to use these funds through their Integrated Plans (IPs) and annual updates. The IPs and annual updates are approved by the county board of supervisors and submitted to the Department of Health Care Services.
For housing developers and service providers, the most important step is to work closely with county behavioral health departments so that certain strategies and services are included in the county’s IP. For more information on how to get involved, see How can housing developers and homelessness providers participate in BHSA planning?.
BHSA housing intervention funding can be used for:
- Capital development: acquisition, construction, or rehab of housing
- Operating costs: keeping housing units stable and affordable
- Supportive services: case management, behavioral health care, and tenancy supports
For projects already funded through Homekey+ or the Behavioral Health Continuum Infrastructure Program (BHCIP), BHSA is especially important. Homekey+ and BHCIP primarily fund the buildings and infrastructure, but don’t necessarily cover the services and operations needed to keep projects stable long-term. BHSA can potentially fill those funding gaps. However, it is recognized that the timing is tricky, as these infrastructure projects may be underway while the new BHSA plans won’t take effect until July 2026. That mismatch means some projects could be up and running before BHSA dollars are available to ensure funding for services or other supports, leaving a funding gap.
Still, this is a major opportunity. Demonstrating how BHSA funding can keep existing or upcoming projects running by covering services, filling operating cost gaps, or ensuring sustainability is critical. Counties must make every dollar stretch — so projects or other services that leverage other state or private funding, fill a clear community need, and demonstrate strong partnerships could have a strong chance of being considered.
How much will my county receive in BHSA funds?
The amount of BHSA funding your county receives depends on various factors, including population size. For BHSA housing intervention dollars, DHCS estimates the total annual statewide housing component will be approximately $950 million to be distributed among all counties for FY 2026-27. DHCS released example county estimates for BHSA housing interventions based on county size:
- Very Large (Population 9.6 million): Los Angeles $254.09 million
- Large (Population 1.6 million): Sacramento, $34.99 million
- Medium (Population 263K): Santa Cruz $6.79 million
- Small (Population 133K): Humboldt $3.3 million
It’s important to note that funding levels fluctuate each year because they are tied to a variable revenue stream — a millionaire’s tax that voters approved in 2004 to support mental health services. Counties must account for this uncertainty when developing Integrated Plans and committing to projects with ongoing costs.
How does BHSA intersect with other funding sources, like Transitional Rent?
BHSA dollars are intended to complement existing funding streams and interventions like Transitional Rent or local flex pools. It can help fill funding gaps for housing supports, tenancy services, or capital projects. However, counties must first use Medi-Cal housing-related services if the local Medi-Cal Managed Care Plans (MCPs) offer them. BHSA funds can only be used if MCPs decline to provide services, the individual is ineligible, or if their benefits have been exhausted.
Because of this, ongoing communication between housing developers, homelessness service providers, county behavioral health departments, and MCPs is essential. Early coordination can align funding sources, prevent service gaps, and ensure housing units are paired with the right supportive services — maximizing the impact of BHSA and Medi-Cal dollars. Without early collaboration, services could be delayed, underfunded, or missed entirely.
Divya Shiv is a senior policy advocate focused on homelessness at Housing California. Adriana Ramos-Yamamoto also contributed to this publication.

