
Access to health care is essential for everyone to be healthy and thrive. In California, Medi-Cal, the state’s Medicaid program, provides free or low-cost health care to over one-third of the state’s population. Medi-Cal covers a wide range of services to Californians with modest incomes, and many children, seniors, people with disabilities, and pregnant individuals rely on it. About half of Medi-Cal beneficiaries are Latinx, highlighting Medi-Cal’s role in promoting health equity.
California’s shortage of health care workers undermines the availability and quality of care for communities across the state. When people can’t find a provider in their area or experience long wait times for appointments, they don’t have meaningful access to health care. Enrolling in Medi-Cal and navigating the health care system can also be difficult, underscoring the need to invest in outreach and enrollment supports. While state policymakers have made considerable investments in recent years to bolster the health care workforce, more progress is needed.
what is health equity?
When everyone has the opportunity to be as healthy as possible and no one is disadvantaged from achieving this because of their race, gender identity, sexual orientation, the neighborhood they live in, or any other socially defined circumstance.
This year, policymakers had to make challenging decisions about health care investments due to the state’s recent budget shortfall and resistance from some state leaders to raise ongoing revenues. This has led to debates over the allocation of revenue from the state’s recently approved Managed Care Organization (MCO) tax. In response, many representatives of the health care industry have proposed Proposition 35, which would:
- Require the state to request federal approval for the MCO tax on an ongoing basis.
- Allocate MCO tax revenue for certain health care investments.
There are merits to having dedicated funding to invest in the state’s health care system. However, this approach would reduce flexibility in the state budget and could negatively affect available funding for other key services that improve the lives of Californians. This Q&A provides a high-level overview of Prop. 35, including how Californians with low incomes might be impacted by its passage as well as implications for the state budget.
table of contents
- What is the Managed Care Organization (MCO) tax?
- How do policymakers currently plan to use MCO tax dollars?
- How does Prop. 35 differ from the current MCO tax plan?
- Would Prop. 35 actually make the MCO tax permanent?
- How would Prop. 35 impact the state budget?
- How would Prop. 35 impact Californians?
- What are arguments for and against Prop. 35?
What is the Managed Care Organization (MCO) tax?
Managed Care Organizations (MCOs), also known as health insurance plans, are responsible for managing health care services as a way to control costs, utilization, and quality of care. Anthem Blue Shield and Kaiser Permanente are two examples of MCOs in California. These health insurance plans oversee the health care benefits that people receive, often requiring prior authorization or referrals to ensure that people receive appropriate and cost-effective care.
MCOs manage health care services for people with private health insurance as well as Medi-Cal enrollees. They contract with Medi-Cal to receive payments based on the number of Medi-Cal recipients they serve. Medi-Cal is a joint federal-state program, with the federal government covering part of the cost and the state covering the rest.
Federal law allows states to impose a tax on MCOs and other health-related services to help cover the state share of Medicaid health care costs, but states must comply with federal regulations and receive federal approval for these taxes. Eighteen states reported having an MCO tax in place during the 2023 state fiscal year.
California’s MCO tax is a charge based on enrollment in Medi-Cal managed care plans and private health insurance plans. The MCO tax is distinct from other types of state taxes in that the primary state fiscal benefit comes from the additional federal dollars drawn down as a result of the tax. MCOs bear very little of the cost, as they receive Medi-Cal payments from state and federal funds that offset the portion of the tax levied on Medi-Cal enrollment. By drawing down additional federal funding, the MCO tax frees up state General Fund dollars that would otherwise have been used to support existing Medi-Cal services.
California’s MCO tax was most recently approved in December 2023, and it will expire at the end of 2026 unless it is renewed again. However, state leaders are seeking additional changes to the MCO tax structure to draw down more federal funding. These changes are still pending federal approval.
The state is expected to receive net revenues of $7 billion to $8 billion annually while the tax is in effect, assuming the federal government approves recent changes. Essentially, the net revenues are the additional federal funds the state is able to draw down minus the cost of the state’s portion of payments to MCOs to offset the cost of the tax. Under the enacted 2024-25 budget, most of that revenue will be used to offset state General Fund spending on existing Medi-Cal services, with a smaller portion going to increased provider rates and augmentations.
Stay in the know.
Join our email list!

How do policymakers currently plan to use MCO tax dollars?
Policymakers outlined a plan — which Prop. 35 would overturn — to use revenue from the MCO tax in the 2024-25 budget package, with the majority of dollars allocated to offset General Fund spending on Medi-Cal and maintain existing services in the program. Assuming that the federal government approves the changes to the MCO tax that state leaders are seeking, the budget includes the following MCO tax dollars to sustain existing services in Medi-Cal:
- $6.9 billion in 2024-25
- $6.6 billion in 2025-26
- $5.0 billion in 2026-27
Policymakers also allocated funding from the MCO tax for new targeted Medi-Cal provider rate increases as well as other investments. These budget allocations include:
- $133 million in 2024-25
- $728 million in 2025-26
- $1.2 billion in 2026-27
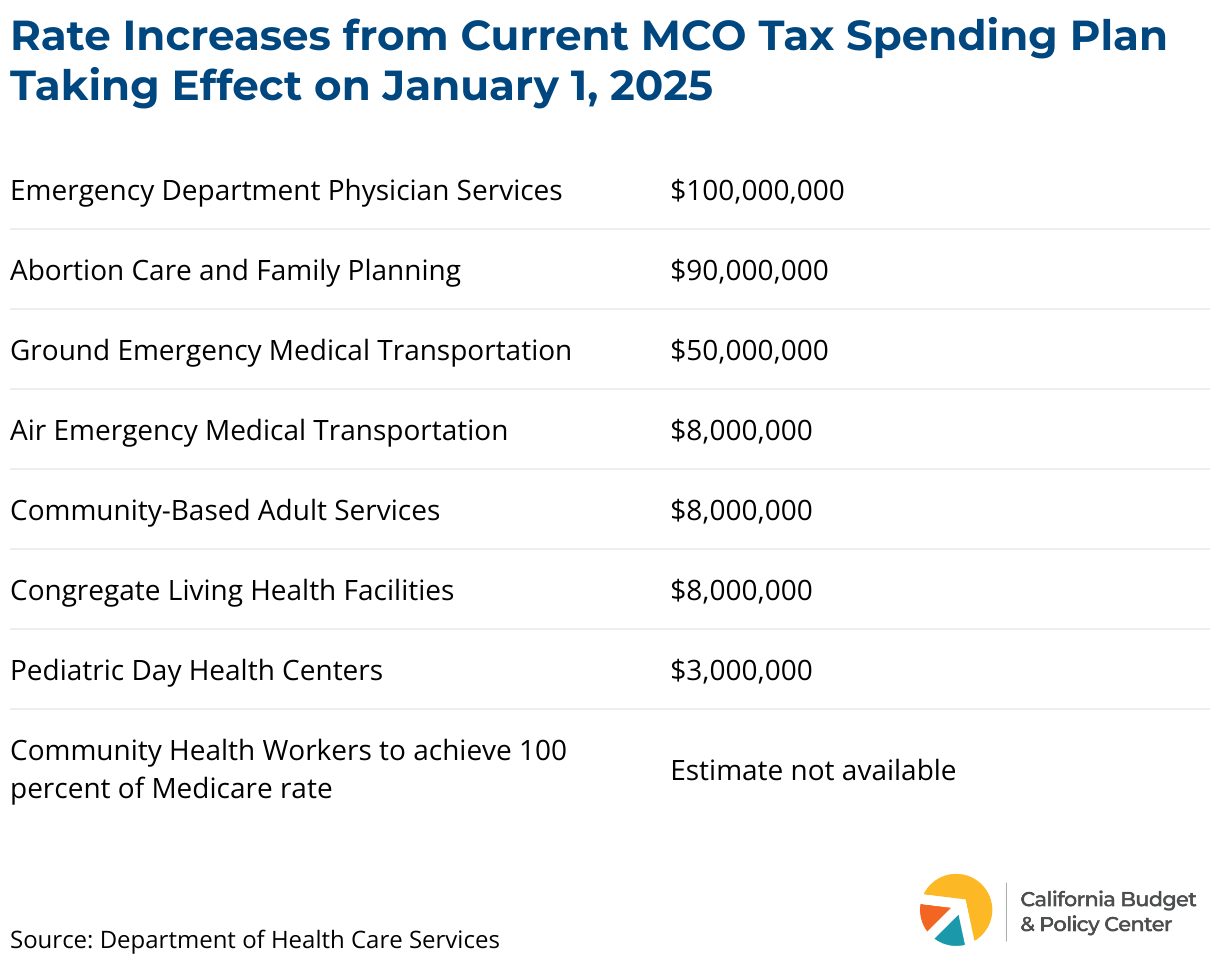
The rate increases from the current MCO tax spending plan are intended to build on investments that policymakers made in previous years. As shown below, the majority of funds for rate increases that will go into effect on January 1, 2025 will support emergency department physician services, abortion care and family planning, and ground emergency medical transportation.
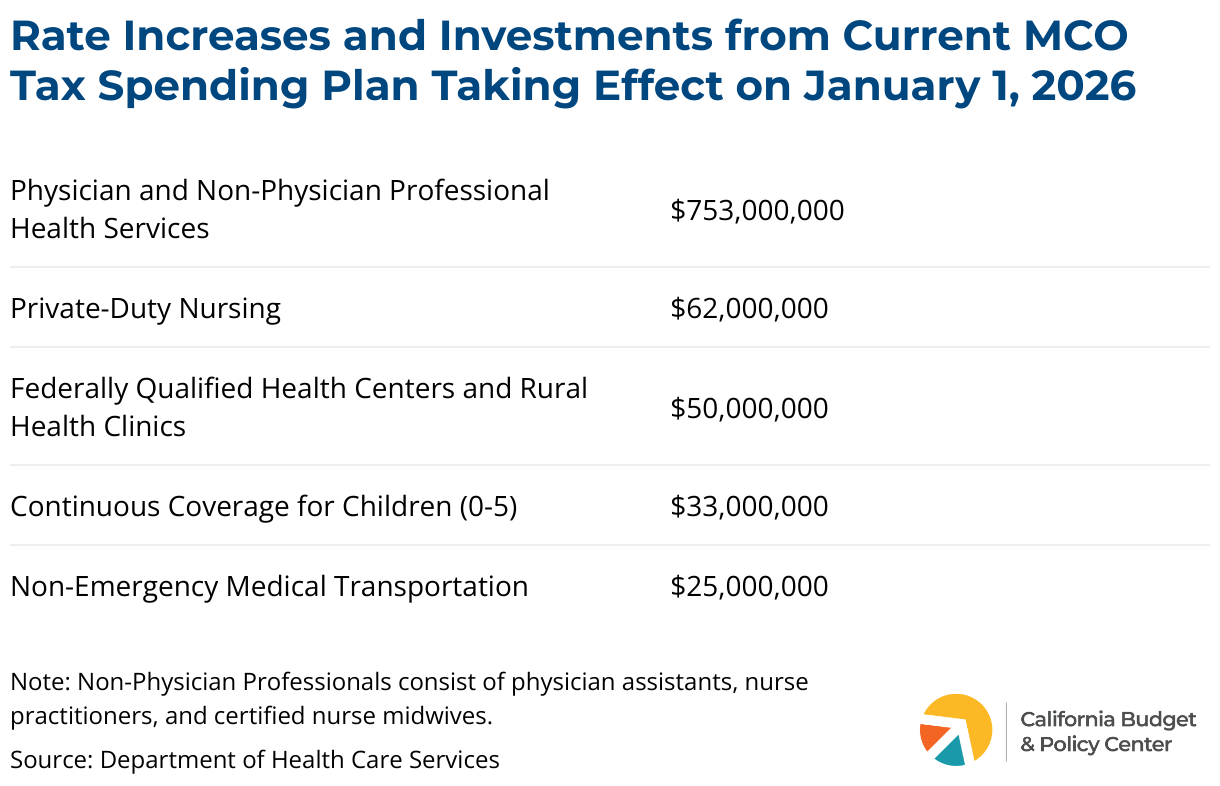
The current MCO tax spending plan also includes additional rate increases and investments that would take effect on January 1, 2026, with the vast majority of dollars allocated to physician and non-physician professionals (e.g., physician assistants, nurse practitioners and certified nurse midwives).
Policymakers also allocated $40 million one-time MCO tax dollars in 2026-27 to strengthen and support the development and retention of the Medi-Cal workforce. This amount reflects a decrease in health care workforce investments that state leaders made in the past. More substantial and sustained investments are necessary to build a health care workforce that can better meet the needs of Californians.
This MCO tax spending plan would be overturned if voters approve Prop. 35.
How does Prop. 35 differ from the current MCO tax plan?
Prop. 35 proposes a major shift to how state policymakers have used MCO tax revenue to essentially reduce, or offset, General Fund spending on Medi-Cal. If passed, Prop. 35 would overturn the current MCO tax spending plan that policymakers agreed upon in the 2024-25 budget.
Prop. 35 would require the California Department of Health Care Services to request federal approval for the MCO tax on an ongoing basis in an attempt to make this funding stream more permanent. Federal approval is required for the state to levy health care taxes that draw down additional federal dollars.
While Prop. 35 provides some flexibility for the state to structure future versions of MCO tax proposals to comply with federal regulations and ensure federal approval, it does set limits to the tax on commercial enrollment. This limitation could affect the state's ability to secure future approval for a tax that generates the same level of revenue as the current tax. The measure also specifies that the MCO tax would not go into effect if the state does not receive federal approval and federal funding in the future.
Additionally, Prop. 35 would establish rules for how MCO tax revenue would be spent in the short term (2025 and 2026) and long term (2027 and beyond). The key difference is that policymakers would no longer be able to use the bulk of the dollars to offset General Fund spending in Medi-Cal. Another notable difference is that Prop. 35 would require funds to be spent by the end of each calendar year or fiscal year, beginning 2027. Currently, policymakers have the flexibility to save funds for future years to help cover costs if the MCO tax is not approved in the future.
If passed, funds would first cover a portion of MCOs’ cost of the tax as well as administrative costs.
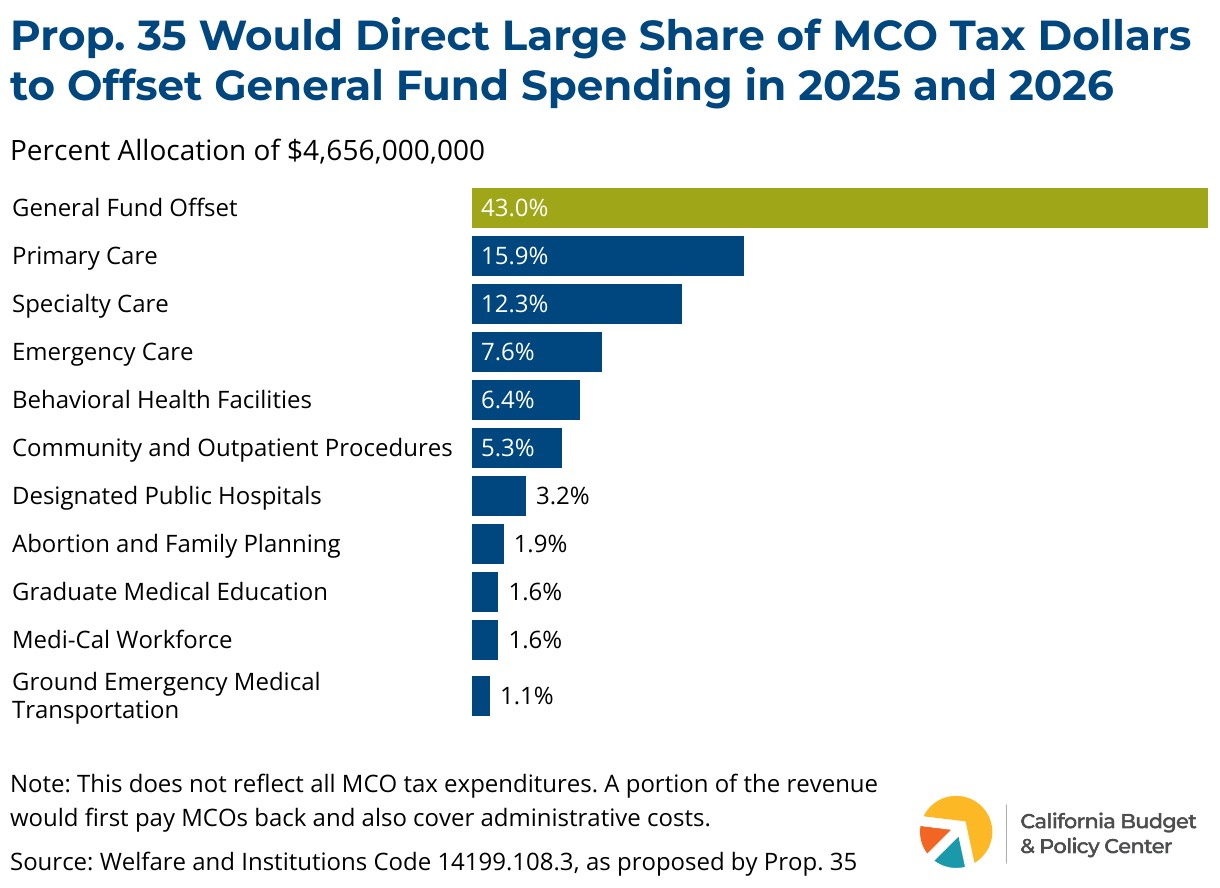
For calendar years 2025 and 2026, $2 billion would be used to offset General Fund spending in Medi-Cal. Specifically, this amount would cover a portion of the non-federal share of Medi-Cal managed care rates for health care services for children, adults, seniors, and people with disabilities. This represents the majority of funds (about 43%), as shown below. MCO tax revenue would also support health workforce initiatives, including primary care, specialty care, and emergency care.
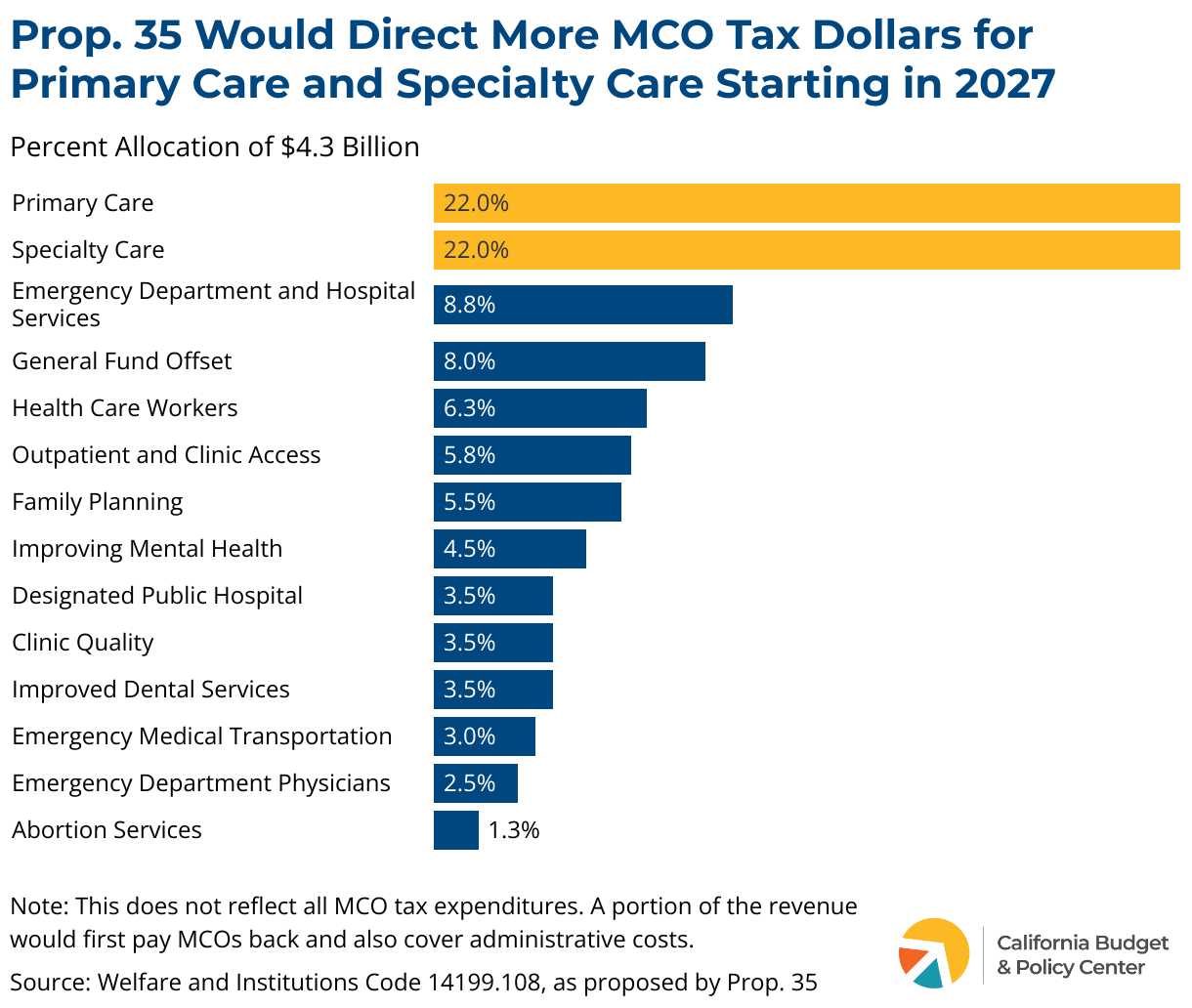
For calendar year 2027 and beyond, Prop. 35 would allocate revenue from the MCO tax differently. After covering a portion of MCOs’ cost of the tax as well as administrative costs, the next $4.3 billion collected from the tax would be allocated for specific purposes. The majority of funds (44%) would support access to primary care and specialty care. Specifically, it would increase reimbursement rates for primary care services and increase the number of specialty care service providers. A smaller portion of funds would support other rate increases, such as emergency department services and family planning. Prop. 35 would allow the Department of Health Care Services to allocate 8% of funds — $344 million — to provide overall support to the Medi-Cal program.
If there are remaining MCO tax revenues after these funding allocations are made, the measure contains parameters to allocate the excess revenue. Examples of these other allocations include:
- Additional General Fund offset to support existing services in Medi-Cal.
- A grant program to expand the number of community health workers.
- Supporting the state’s ongoing efforts to reduce the cost of prescription drugs.
- Providing additional funding to health workforce initiatives.
In addition, Prop. 35 would establish oversight and accountability measures, requiring the state controller to perform independent financial audits. It would also create an advisory committee that would provide input to the Department of Health Care Services on future MCO tax proposals. This advisory committee would be made up of mostly health care provider representatives.
Would Prop. 35 actually make the MCO tax permanent?
No, the MCO tax funding structure under Prop. 35 is entirely dependent on federal approval and ongoing renewals. Prop. 35 would require the California Department of Health Care Services to request federal approval for the MCO tax on an ongoing basis in an attempt to make this funding stream more permanent. Federal approval is required for the state to levy health care taxes that draw down additional federal dollars.
One issue with Prop. 35 is that the MCO tax may not be a sustainable, long-term funding source. While the federal government has historically approved California’s MCO tax, it has indicated that it may revise the rules governing state MCO taxes in the future, which would have implications for the amount of net revenue that future versions of the tax may bring into the state.
Without federal approval and federal funding, the MCO tax and spending plan under Prop. 35 would not be implemented.
How would Prop. 35 impact the state budget?
While Prop. 35 would ensure more funding is dedicated for health care, its requirement to spend MCO tax revenues on specific services would also limit policymakers’ flexibility in making budget decisions. This is particularly concerning in years when the state is facing a budget shortfall because the reduced flexibility could lead policymakers to make cuts to other critical public services to balance the budget.
State leaders are required to balance the budget each year, and there are already several strict requirements on how some state funds are spent that make budgeting complex. By creating additional mandates on state spending, Prop. 35 would result in policymakers having even less flexibility in making budget decisions. While the measure gives policymakers some ability to modify the structure and uses of the MCO tax, changes would require a three-fourths vote in the Legislature — which can be difficult to obtain — and would need to further the purpose of Prop. 35.
In years when the state is facing a budget shortfall, this limited flexibility could result in cuts to other critical public services that help Californians make ends meet and address vital needs, such as income supports, subsidized child care, food assistance, and investments in reducing homelessness and increasing affordable housing.
Of course, cuts could be limited or avoided during budget deficits if state leaders are able to raise new revenues to address a shortfall. However, the state Constitution requires a two-thirds vote in the Legislature to raise taxes, while spending cuts can be approved with a simple majority, and state leaders have generally been more inclined to make cuts than to increase taxes.
In the near term, Prop. 35 would result in the recently enacted 2024-25 budget being out of balance. This is because a solution to the budget shortfall involves using some MCO tax dollars that were previously intended to support provider rate increases and other augmentations to instead offset General Fund spending on existing Medi-Cal services. Since Prop. 35 would require MCO tax revenues to be used for health program augmentations instead of offsetting existing spending, state leaders would have to identify other solutions — potentially spending cuts or delays, revenue increases, or additional budget reserve withdrawals — in next year’s budget to cover the difference. The Legislative Analyst’s Office estimates that the General Fund impact would be between $1 billion and $2 billion in 2025 and 2026, but in a legislative hearing on August 13, 2024, the Department of Finance noted that it estimates the impact could range from $2.6 billion and $4.9 billion in fiscal years 2024-25 through 2026-27.
In the long term, raising state General Fund revenues — through sources aside from the MCO tax — would help to increase the state’s capacity to cover the costs of existing Medi-Cal services and improve state health services and increase access to care, without jeopardizing other state services. This is especially important given that there is no guarantee the federal government will continue to approve an MCO tax that yields the amount of revenue anticipated from the currently authorized tax.
Stay in the know.
Join our email list!
How would Prop. 35 impact Californians?
If passed, millions of Californians who receive health care services through Medi-Cal — about half of whom are Latinx — could have better access to care, especially for primary care and specialty health care services. Increasing provider participation in Medi-Cal is critical to improving access to a wide range of health care services, especially in historically underserved areas where there is often a shortage of providers. By increasing the number of providers in the Medi-Cal network, patients can receive more timely care, which can help improve health and well-being for all Californians, but especially Latinx communities.
However, there are some critical health equity investments that are included in the current MCO tax spending plan that are either not included or not prioritized in Prop. 35. Examples include:
- Implementing continuous coverage for children from birth to age five.
- Raising rates for community health workers.
- Investing in long-term supports for children with complex medical needs, older adults, and people with disabilities.
These potential cuts raise health equity concerns, as they would disproportionately impact people of color, children, older adults, and people with disabilities. Policymakers should explore alternative revenue-raising measures to sustain and advance these crucial health equity initiatives, if Prop. 35 passes.
Additionally, Prop. 35’s limitations on using MCO tax proceeds to offset General Fund spending on current Medi-Cal services could make policymakers more likely to make cuts to other state services when facing budget shortfalls. Such cuts would likely harm Californians with low incomes most. For example, in the difficult budget years during and following the Great Recession, deep cuts were made to safety net programs such as subsidized child care, income supports for families under the California Work Opportunity and Responsibility to Kids (CalWORKs) program, and income support for older adults and people with disabilities under the Supplemental Security Income/State Supplementary Payment (SSI/SSP) program.
Lastly, the passage of Prop. 35 would lock in spending decisions in the future, which would impact how Californians engage with the state budget process. Advocates and community members would have less opportunity to weigh in on how state resources should be allocated because the MCO tax spending decisions would be constrained by the ballot measure. Currently, Californians can contribute to conversations about how MCO tax revenue should be spent during the budget process via public hearings and interactions with policymakers.
What are arguments for and against Prop. 35?
Supporters of Prop. 35 believe the measure will protect and enhance access to care for Medi-Cal patients by ensuring that MCO tax dollars are directed toward patient care. They argue that it would prevent lawmakers from redirecting funds intended for health care to other purposes. Key supporters include the California Medical Association, Planned Parenthood Affiliates of California, the California Hospital Association, the California Primary Care Association, and the California Dental Association.
Opponents of Prop. 35 argue that the measure would reduce flexibility in how Medi-Cal dollars are allocated and overturn the commitments made in the 2024-25 budget to fund important services with MCO tax dollars, including continuous Medi-Cal coverage for young children and the rate increase for community health workers. Opposition groups include The Children’s Partnership, the California Pan-Ethnic Health Network, the California Alliance for Retired Americans, Courage California, and the League of Women Voters of California.