Recent federal actions introduced significant changes to the Supplemental Nutrition Assistance Program (SNAP), known as CalFresh in California, via the 2025 Republican megabill, H.R. 1. One of the major changes was to the time limit provision, which expanded the groups of people subject to time limits and eliminated some key exemptions for participants already facing challenges in the labor market.
What Are CalFresh Time Limits?
Adults participating in CalFresh are limited to a three months of food assistance every three years unless they are working, volunteering, or in a work or training program at least 20 hours a week or are otherwise exempted. Time limits refer to the three month in three year rule and hinge on meeting work reporting requirements.
The following facts highlight the people most affected by these changes and at risk of losing their food assistance when these burdensome and bureaucratic work reporting requirements take effect on June 1, 2026. Ensuring people are properly screened for exemptions and eliminating red tape could help avoid a hunger crisis for California families.
1. Nearly 80% of New Time-Limited Adults Could Lose Their Food Assistance
According to recent estimates released by the Legislative Analyst’s Office, H.R. 1 will make 840,000 California adults newly subject to CalFresh time limits. Changes to CalFresh time limits include:
Tightening rules for area waivers based on economic conditions, which recognized limited job availability.
- Extending time limits to adults through age 64, rather than 54;
- Extending time limits to adults caring for children 14 and older;
- Eliminating exemptions for former foster youth, veterans, and people experiencing homelessness;
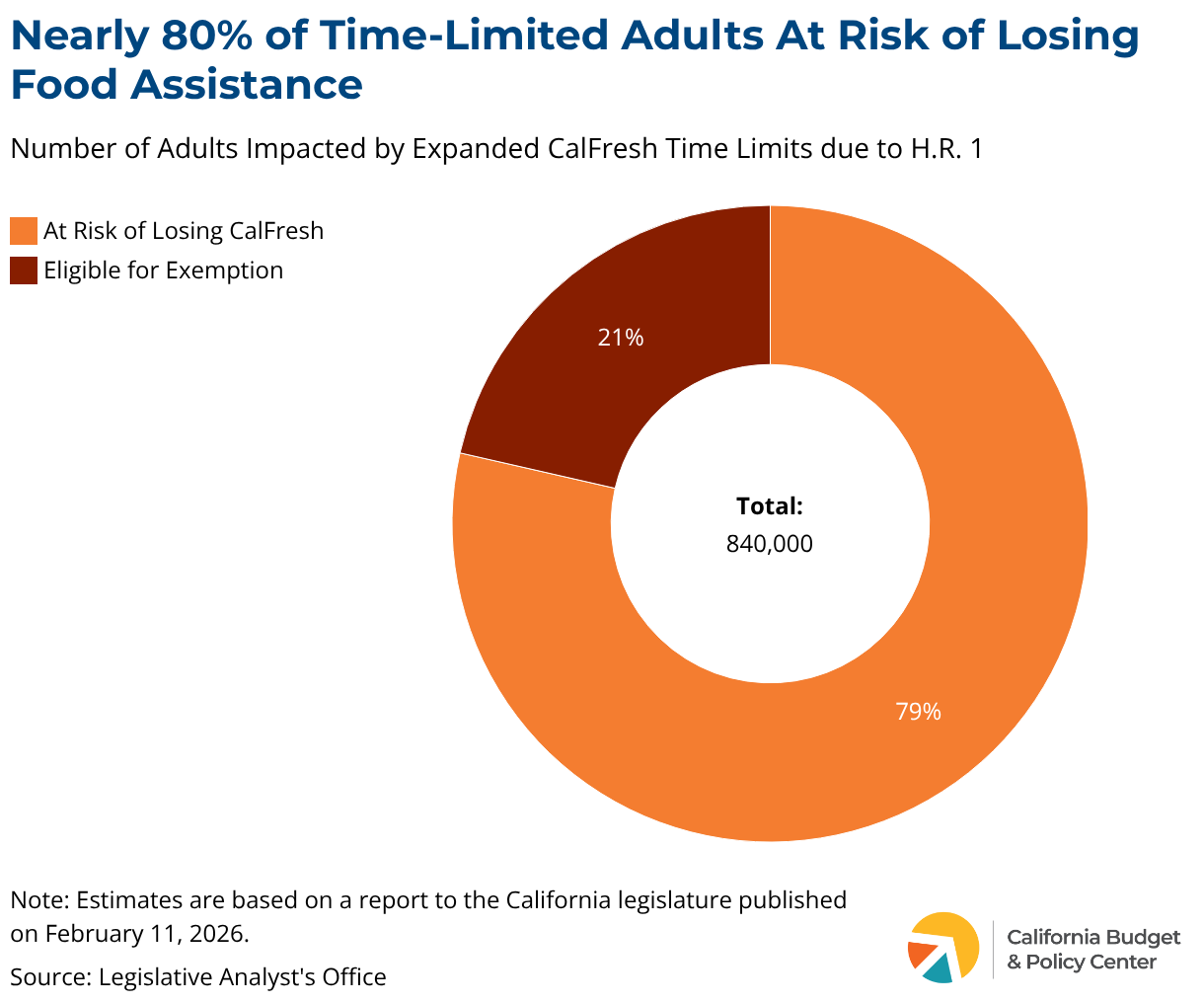
The California Department of Social Services estimates that nearly 80% of these newly time-limited adults will not qualify for an exemption. Those who do not qualify for an exemption are at risk of losing their food assistance, as many SNAP recipients have low-wage and unstable jobs. These jobs are often characterized by irregular schedules, where people may not be able to meet specific work hour requirements if their hours are cut or they miss work due to illness. Additionally, those who meet the work criteria are still at risk of losing their benefits due to administrative barriers, such as difficulty completing complex paperwork, missing deadlines, or lacking the necessary documents to prove eligibility.
2. Time Limit Expansion Puts Older Adults and Parents of Older Children At Risk
H.R. 1 expanded the age limit for people subject to time limits to adults up to age 64. Additionally, for the first time, it also expanded time limits to parents of children over the age of 13. In total, this puts over 250,000 adults and their families at risk of losing their monthly food assistance.
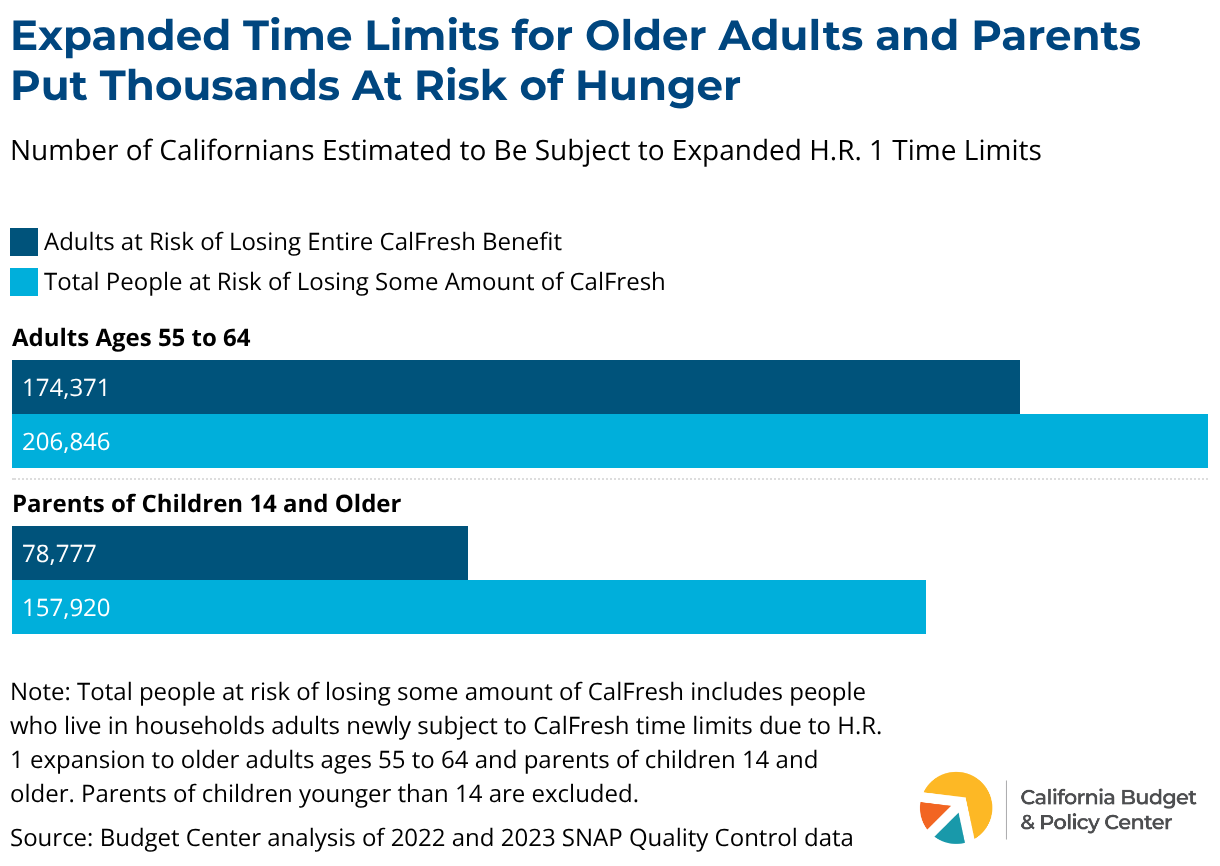
Research by the National Academies of Sciences, Engineering, and Medicine shows that age discrimination in the workforce is a core challenge for older adults seeking employment and that adults in their early 60s are less likely to find new employment after separating from their previous job. The CalFresh time limits put harsh time pressures on Californians who face significant unemployment spells and barriers to employment.

3. Veterans, Former Foster Youth, and People Experiencing Homelessness Could Lose Food Assistance
H.R. 1 eliminated three exemptions to time limits that helped veterans, former foster youth, and people experiencing homelessness maintain their food assistance beyond the three-month time limit. The former policy recognized that the exempted populations often face increased challenges to maintaining stable employment due to health challenges and limited opportunities.
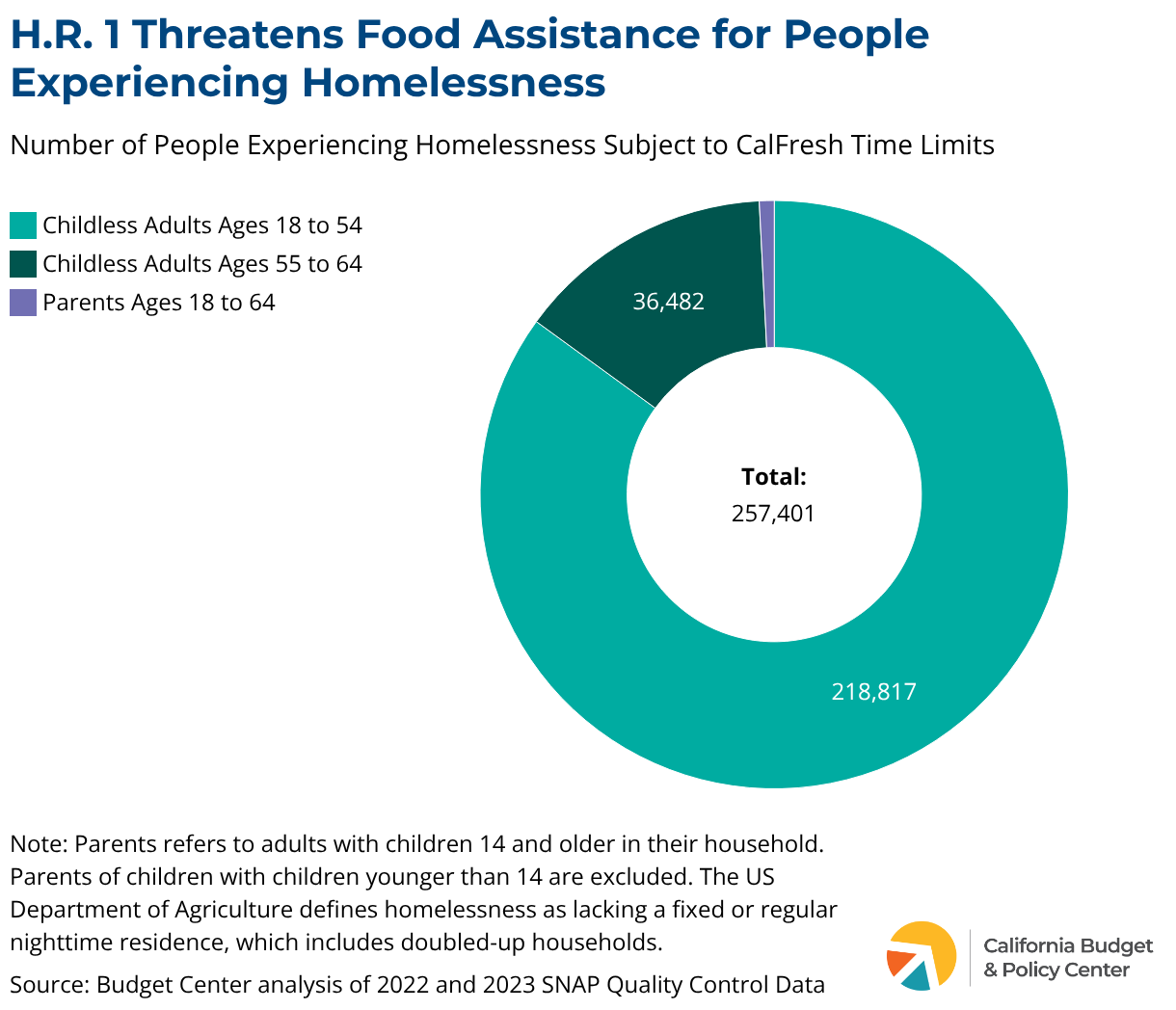
While the data is too limited to estimate the number of impacted veterans and former foster youth, over 257,000 Californians experiencing homelessness will be at risk of losing their CalFresh monthly benefit. Nearly all of these participants are childless adults, who are typically already excluded from most other safety net programs. Additionally, research shows that people experiencing homelessness have disproportionately higher rates of disabling conditions, which are especially high among the older adult population who are newly subject to the time limits.
Research using data from the California Interagency Council on Homelessness, Homeless Data Integration System, shows that significantly fewer unhoused Californians have access to both CalFresh and housing services due to SNAP’s more expansive definition of who is experiencing homelessness. Given this, people experiencing homelessness by SNAP’s definition, who do not fit under the traditional US Department of Housing and Urban Development definition, could be at greater risk of losing their primary source of assistance.
4. The Large Majority of Newly Time-Limited Adults Live in Deep Poverty
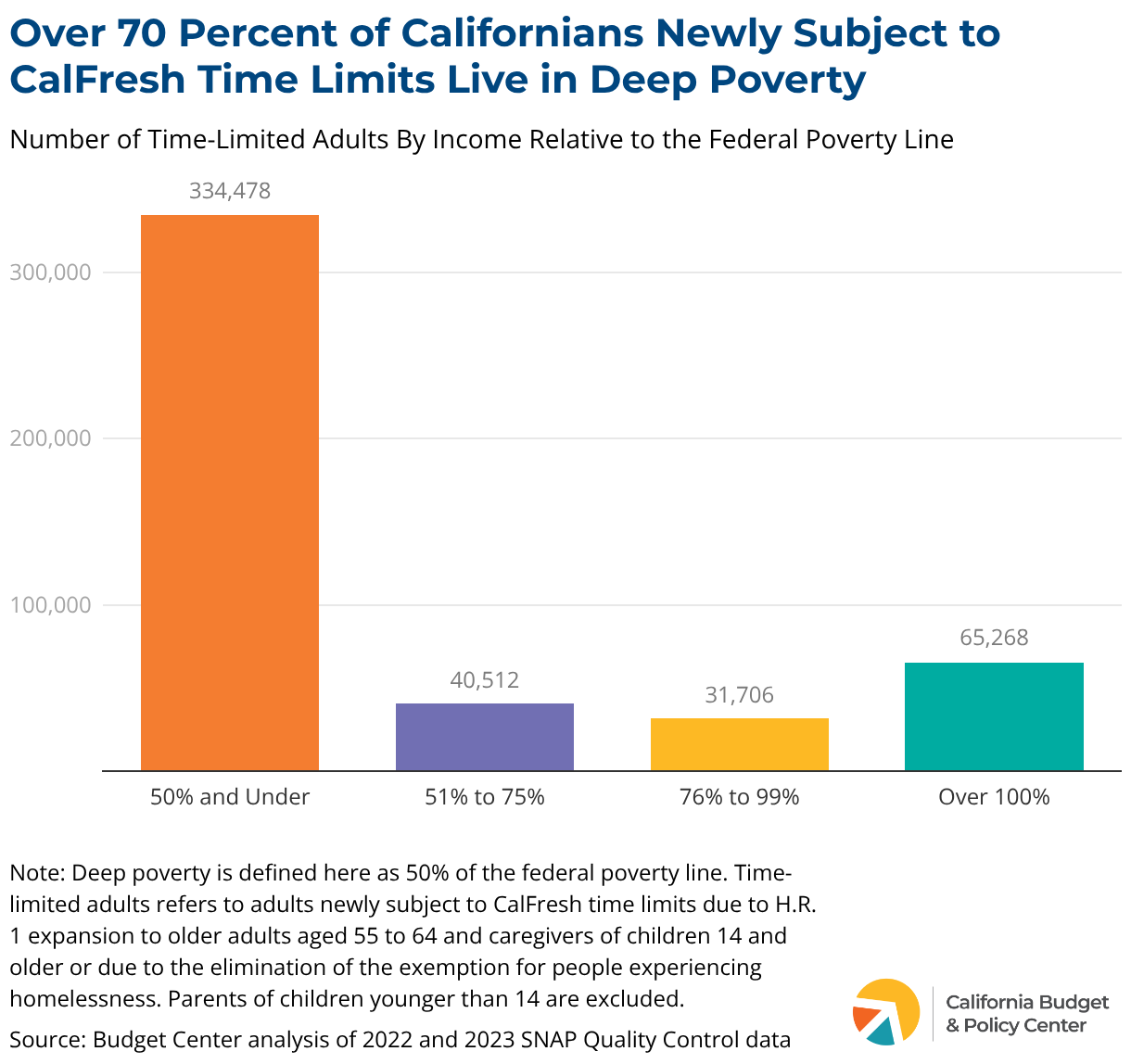
Newly time-limited adults — including older adults, parents, and people experiencing homelessness — predominantly live in deep poverty, defined as 50% of the federal poverty line or an income less than $7,980 per year for a one-person household. Given their extremely low incomes, CalFresh is likely to be a sizeable monthly support for those experiencing deep poverty. As a result, any disruption to their food assistance — due to red tape in paperwork requirements or if their working hours decrease due to their employer or a health emergency — could be the difference between eating and not eating.
Food insecurity is closely tied to negative health outcomes and even increased mortality rates among adults. For households that already have very low incomes and face barriers to meeting their basic needs, being able to eat is essential to ensuring people are even able to seek out employment.
5. Children and People With Disabilities Stand to Lose Household Benefits
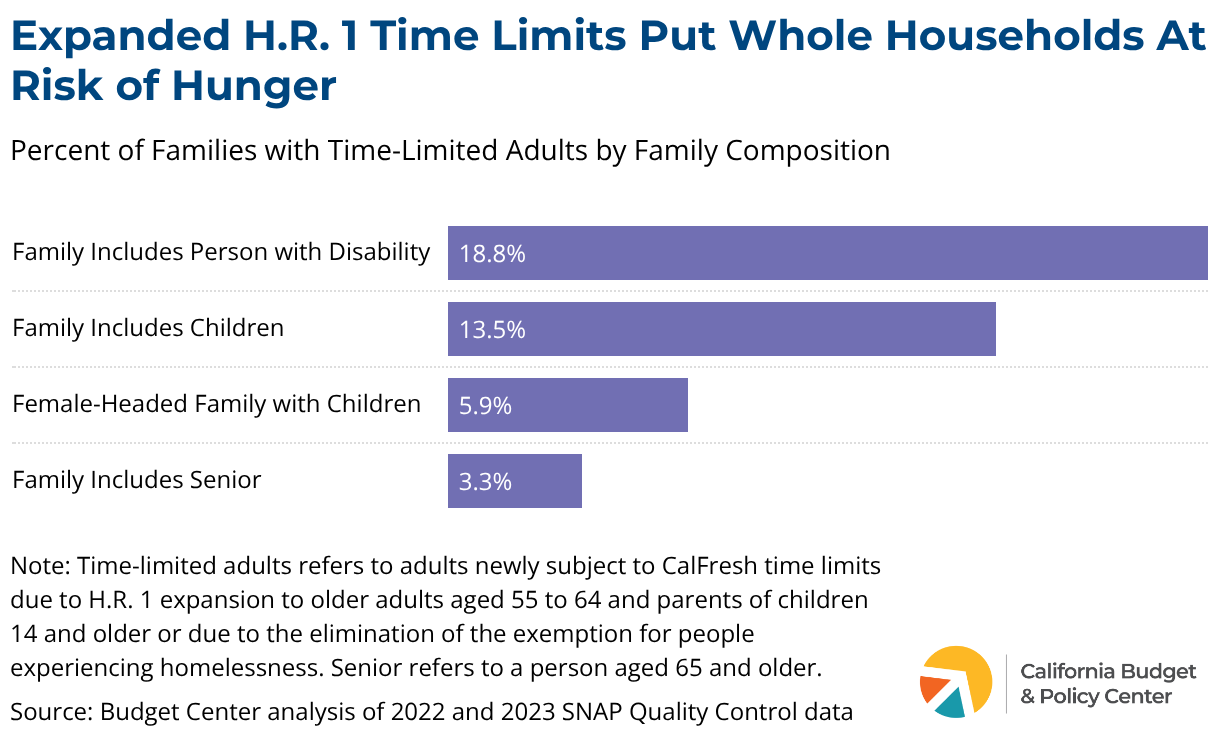
While time limits are specifically imposed on adults without disabilities, the threat to their CalFresh assistance puts pressure on their entire families’ food budgets. Nearly 20% of households with adults newly subject to time limits include a person with a disability, and over 13% of families include children. If the adult subject to time limits loses access to CalFresh, the rest of the family may still be eligible for a reduced monthly benefit, but would face significant challenges meeting their needs if the time-limited adult’s portion of the benefit is taken away.
Despite the intended effort to push CalFresh participants into sustained employment, time limits, which more often push people off assistance entirely, will take food away from children, seniors, and people with disabilities.
Conclusion
The majority of SNAP recipients who can work already do. Those who cannot work face significant barriers to employment, such as disability, caregiving responsibilities, or macroeconomic conditions outside their control, such as a lack of job opportunities. Rather than fostering economic mobility, layers of paperwork needed to avoid program time limits threaten to take away food from people in deep poverty, including children, seniors, people with disabilities, and people experiencing homelessness.
As California moves to implement the expanded CalFresh time limits, state leaders should push for adequate resources so that administering agencies can comprehensively screen people for exemptions and try to prevent as many people from falling off CalFresh due to new bureaucratic barriers imposed by Congress and the Trump administration.
Monica Davalos contributed to this publication.