Read this publication in English.
Conclusión clave
Las demandas de desalojo en California han alcanzado su nivel más alto en seis años; sin embargo, la mayoría de los inquilinos enfrentan el proceso solos y sin apoyo legal. Los programas estatales están lejos de satisfacer la necesidad existente y, sin una inversión sostenida y un compromiso estatal con la defensa legal, más californianos perderán sus viviendas y quedarán en la calle.
Todos los californianos merecen un lugar seguro donde vivir, y eso requiere protecciones sólidas para los inquilinos y acceso a defensa legal, independientemente de sus ingresos o antecedentes. La defensa legal en casos de desalojo, junto con la educación, la mediación y la intervención temprana, son herramientas comprobadas para evitar que las personas pierdan su vivienda, reducir la inestabilidad habitacional y proteger las familias de problemas a futuro. Sin embargo, mientras las demandas de desalojo continúan aumentando y millones de californianos de bajos ingresos enfrentan altos costos de vivienda junto con amenazas a su cobertura médica y a la asistencia alimentaria. Los líderes estatales pueden hacer mucho más para garantizar que los californianos puedan permanecer en sus hogares.
Este informe se basa en A Civil Injustice: The State of Eviction in California (Una injusticia civil: examina las principales tendencias de los desalojos formales en California, explica los programas estatales y el financiamiento destinados a la defensa contra desalojos, y presenta recomendaciones de medidas pública que los líderes estatales pueden implementar para mantener a los inquilinos en sus viviendas, promover la estabilidad habitacional y prevenir que las personas queden en la calle.
Para obtener más información sobre el proceso de desalojo de California, vea The Pipeline, una herramienta de aprendizaje interactivo. Siga a un inquilino que pasa por el sistema de desalojo de California para ver cómo las barreras procesales expulsan a las familias de sus hogares antes de que puedan ver a un juez.
Acerca de este informe
Este informe fue escrito en colaboración por Kyle Nelson, director de investigación y política en Strategic Actions for a Just Economy (SAJE), y Francisco Dueñas, director ejecutivo de Housing Now!/ ¡Vivienda Ahora!.
Strategic Actions for a Just Economy (SAJE) es una organización de base comunitaria y de defensa de derechos con sede en Los Ángeles que trabaja para promover la justicia económica en comunidades de color de bajos ingresos. SAJE colabora con inquilinos, trabajadores y miembros de la comunidad para fortalecer el poder colectivo, combatir el desplazamiento y promover políticas que amplíen el acceso a viviendas asequibles, empleos de calidad y vecindarios saludables. A través de la organización comunitaria, la incidencia en políticas públicas y el desarrollo de liderazgo, SAJE desempeña un papel fundamental en la formulación de iniciativas locales y estatales destinadas a proteger a los inquilinos y fortalecer la estabilidad de la vivienda.
Housing Now!/ ¡Vivienda Ahora! es una coalición de defensa de derechos a nivel estatal dedicada a promover políticas e inversiones para hacer frente a las crisis de la vivienda asequible y la falta de hogar en California. La coalición reúne a organizaciones dedicadas a la vivienda, la salud, el trabajo y las iniciativas comunitarias con el fin de impulsar un aumento de la financiación estatal, una mayor protección de los inquilinos y soluciones a largo plazo que amplíen el acceso a viviendas asequibles. Housing Now! desempeña un papel fundamental en la definición de las prioridades presupuestarias y políticas del estado, centrándose en garantizar que los recursos lleguen a las comunidades más afectadas por la inestabilidad de la vivienda.
1. Los desalojos están aumentando en California a pesar de las protecciones disponibles para los inquilinos
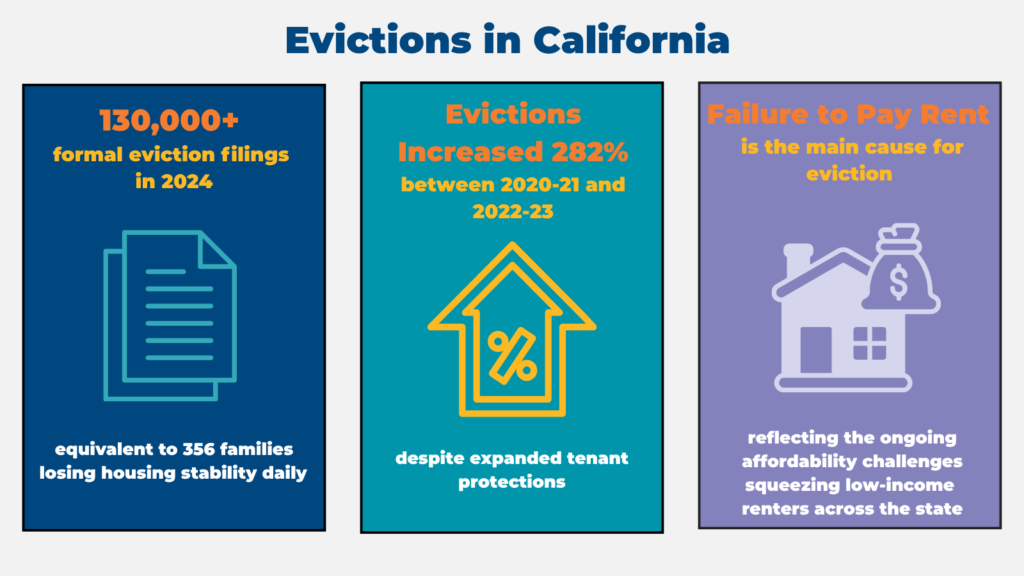
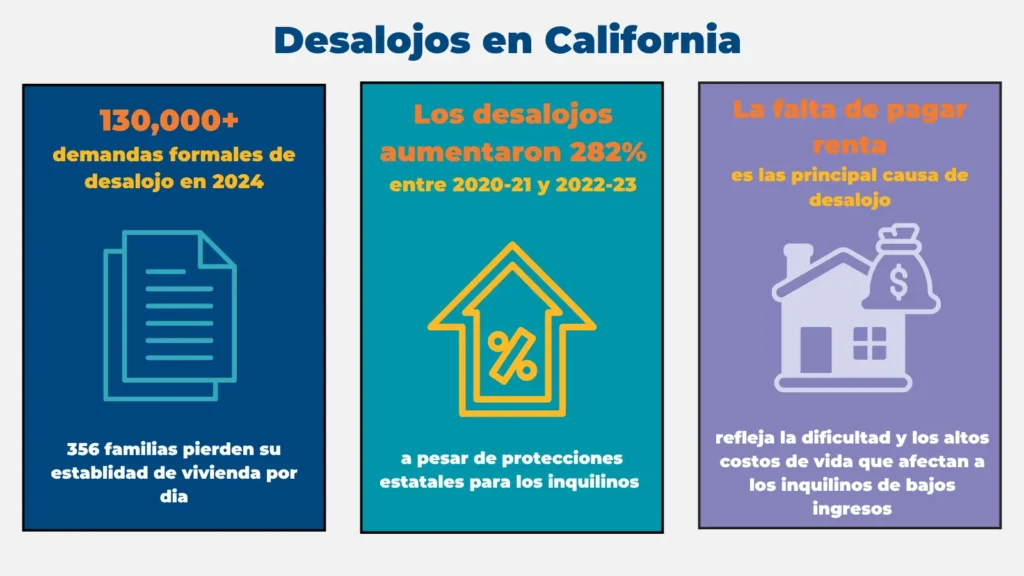
En 2024 se presentaron más de 130 mil casos de desalojo formal en California, y la cantidad de demandas de desalojo durante los últimos dos años ha sido la más alta de los últimos seis años, superando los niveles previos a la pandemia a pesar de las protecciones estatales y locales disponibles para los inquilinos.
Detrás de cada demanda de desalojo hay una familia o una persona en riesgo de perder su vivienda, así como su estabilidad económica, su empleo y sus vínculos comunitarios. Las ramificaciones de esto afectan con mayor dureza a los californianos de bajos ingresos y a las mujeres de color, en especial a las mujeres afroamericanas, quienes enfrentan desalojos de manera desproporcionada debido al persistente legado de las políticas de vivienda racistas y las prácticas discriminatorias que durante mucho tiempo han limitado el acceso de las comunidades de color a viviendas estables y asequibles, así como a la seguridad económica.
Según el informe de SAJE, las demandas formales de desalojo en California subieron un 282% entre los años fiscales 2020–21 y 2022–23, y la cantidad de demandas en los años fiscales 2022–23 y 2023–24 es la más alta en seis años, superando los niveles anteriores a la implementación de la Ley de Protección de Inquilinos (Tenant Protection Act) (TPA) a pesar de estas nuevas protecciones estatales. La TPA exigió que los propietarios tuvieran una “causa justificada” para desalojar a un inquilino y estableció un límite estatal al aumento de renta aplicable a la mayoría de los propietarios de viviendas residenciales. Si bien estas salvaguardas y protecciones son importantes para proteger a los inquilinos y los costos de vivienda que enfrentan, lamentablemente hacen poco por quienes afrontan un desalojo formal. La TPA no cerró las brechas legales que permiten a los propietarios aumenten los costos de vivienda mediante otros cargos arbitrarios y sigan imponiendo aumentos de alquiler significativos que pueden causar dificultades económicas y derivar en desalojos.
La falta de pago de renta continúa siendo la causa más común de los desalojos formales, lo que refleja las dificultades que los inquilinos de bajos ingresos enfrentan en el estado. Sin embargo, las demandas de desalojos formales reflejan sólo una parte de la situación. Muchas más personas en California son desalojadas de manera informal, sin un registro judicial, lo que significa que la verdadera magnitud de los desalojos probablemente sea mucho mayor de lo que muestran los datos.
2. Muchos inquilinos enfrentan su desalojo sin ayuda, y en California faltan datos para entender plenamente el alcance de la situación
Cuando los inquilinos de California enfrentan un desalojo formal, la mayoría lo hacen sin ayuda. A diferencia de los demandados en el sistema de justicia penal, los inquilinos de California no tienen garantizado el derecho a representación legal porque sus casos avanzan en el sistema de justicia civil. Esto ocurre a pesar de la evidencia que demuestra que las intervenciones preventivas y legales son una forma rentable y eficaz de ayudar a las personas a permanecer en sus hogares.
California carece de un sistema estatal integral para dar seguimiento a los desalojos. Además, los datos disponibles no incluyen los desalojos informales. La información disponible proviene directamente de cada uno de los 58 condados de California, todos los cuales tienen sus propios métodos para documentar los resultados y poner esa información a disposición del público, si es que lo hacen.
Las investigaciones de SAJE destacan importantes deficiencias en los datos de los resultados de los desalojos, o datos consistentes, en especial en los condados grandes como Los Ángeles, Riverside, Sacramento, San Diego y San Francisco. Esto es preocupante ya que contienen ciudades con grandes poblaciones de inquilinos, mercados de vivienda de precios elevados y la mayor cantidad de demandas de desalojo.
Estas brechas indican que California no cuenta con una comprensión plena de los resultados de los desalojos y la gente que queda sin hogar. Por esta razón, la verdadera escala y los efectos de los desalojos, en especial los informales, seguramente son mucho mayores que los sugeridos por los datos actuales.
3. Casi la mitad de los californianos pierde su caso de desalojo antes de ver a un juez
Según los registros de desalojo disponibles, más del 46% de los casos concluye con una sentencia en rebeldía, lo cual significa que los inquilinos pierden antes de ver a un juez.. Las sentencias en rebeldía ocurren cuando un inquilino no presenta una respuesta formal a la demanda de desalojo formal del propietario dentro del plazo obligatorio o no se presenta en el tribunal. Casi todos estos fallos en rebeldía (96 %) ocurren en esta etapa inicial, cuando el inquilino no responde a la demanda de desalojo, antes incluso de que se programe una audiencia. Esto suele ocurrir por una falta de acceso a apoyo legal, procesos complejos y difíciles de entender, una imposibilidad de ausentarse al trabajo o dificultades de transporte, así como por temor al sistema judicial.
Hasta 2024, los inquilinos tenían solo cinco días para responder; desde entonces, ese plazo se amplió a diez días, lo que podría reducir las tasas de sentencias en rebeldía con el tiempo, aunque aún está por verse el impacto total de este cambio. También es poco común que un caso de desalojo llegue a juicio, ya que aproximadamente el 85 % de los resultados en casos de desalojo se producen antes del juicio, a pesar de que los juicios con jurado suelen ser más favorables para los inquilinos.
4. Los programas de defensa legal contra desalojos en California funcionan, pero no logran cubrir la enorme necesidad
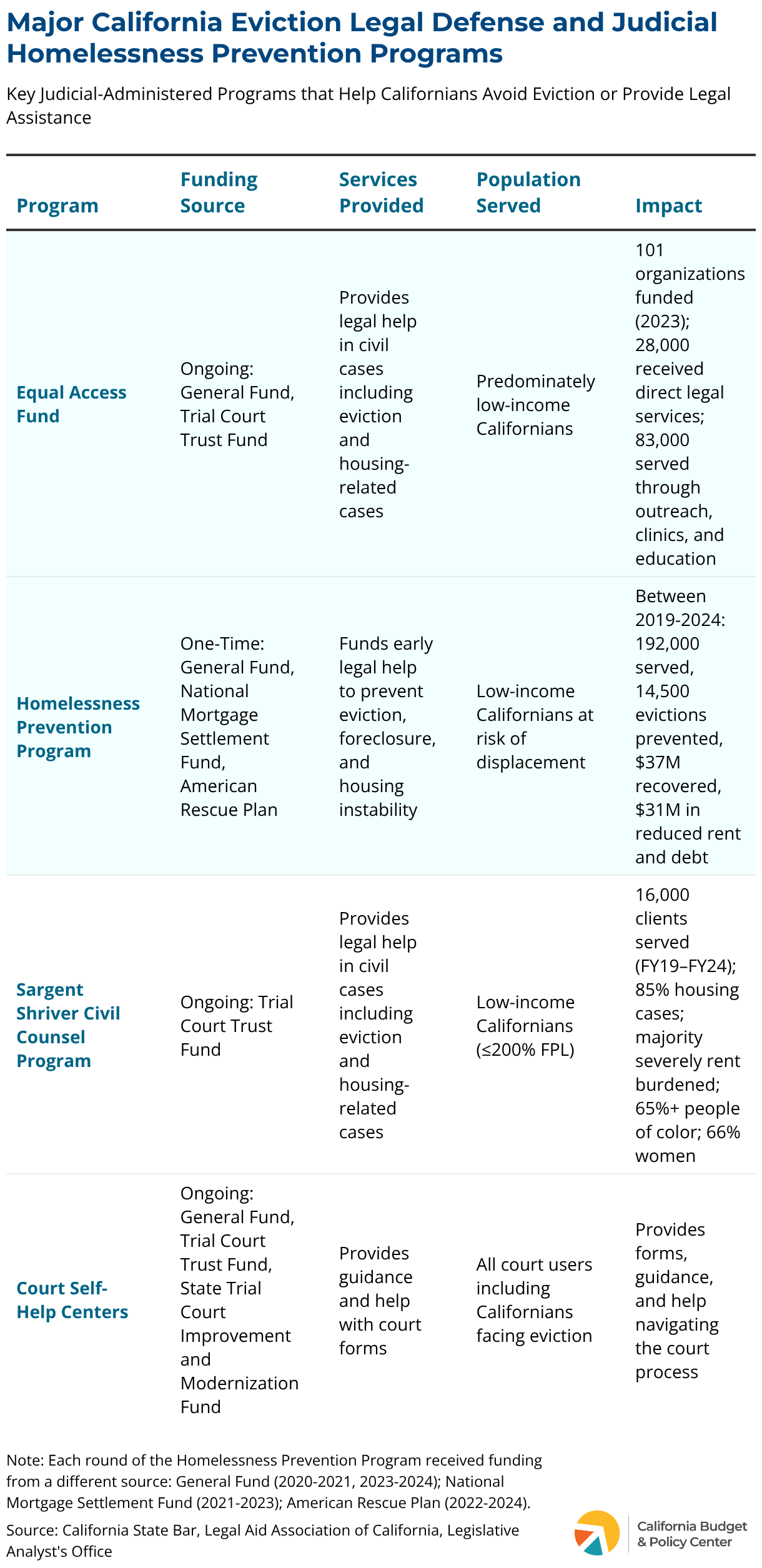
California financia la defensa legal contra desalojos a través de un pequeño conjunto de programas estatales, pero las inversiones están muy por debajo de lo que se necesita. No existe una fuente estatal permanente y exclusiva de financiamiento dedicada únicamente a la defensa legal contra desalojos o a la prevención de la falta de vivienda relacionada con procesos judiciales. En cambio, un pequeño grupo de programas estatales financia este trabajo junto con otros tipos de casos civiles.
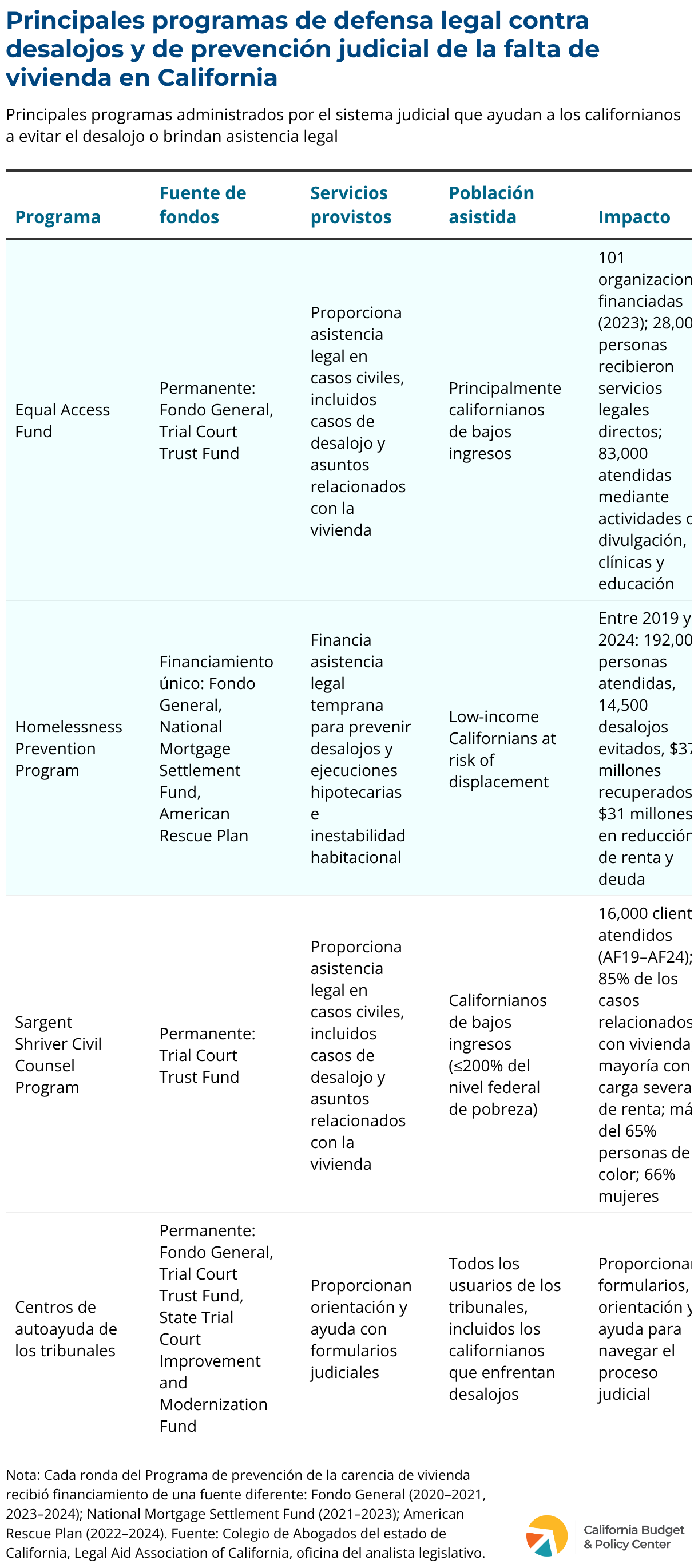
Los principales programas estatales de prevención y defensa legal contra desalojos son:
- Equal Access Fund Program (Programa del Fondo de Acceso Equitativo) (EAF)
- Programa de Prevención de la Carencia de Hogar (Homelessness Prevention Program) (HP)
- Programa de representación legal civil Sargent Shriver (programa Shriver)
- Centros de autoayuda de los tribunales
5. El sistema de defensa contra desalojos en California sigue siendo fragmentado y enfrenta amenazas de financiamiento
Los principales programas estatales han demostrado resultados, pero no alcanzan a cubrir la necesidad de los californianos. El sistema estatal de defensa contra desalojos es fragmentado, limitado en alcance y desigual entre distintas regiones y no ha habido financiamiento estatal destinado específicamente a la defensa legal contra desalojos desde el presupuesto estatal de 2023–24.
Las organizaciones de asistencia legal que proporcionan servicios de prevención de desalojos o defensa legal entre otros dependen de una combinación fragmentada de fondos locales, federales y subvenciones únicas de disponibilidad y alcance variados. Solo existen programas de derecho a contar con representación legal en dos jurisdicciones principales, pero incluso estos se ven limitados por topes de elegibilidad según los ingresos, restricciones geográficas y plazos de respuesta cortos que los inquilinos suelen incumplir.
La red fragmentada de proveedores de defensa legal contra desalojos es solo una parte del panorama. Los programas no judiciales de prevención de la falta de hogar, tales como el programa de asistencia y prevención para personas sin hogar (Homeless Housing Assistance and Prevention) (HHAP) que puede financiar asistencia para el pago del alquiler y otras iniciativas de prevención, también son implementados a través de proveedores diversos con financiamiento igualmente insuficiente. El resultado es un sistema de prevención de la carencia de hogar que deja a muchos inquilinos de California sin recurso cuando se enfrentan a un desalojo.
Simultáneamente, el financiamiento federal de organizaciones de asistencia legal sigue siendo incierto. En el presupuesto federal de 2026, se propuso eliminar por completo el financiamiento federal para la Legal Services Corporation (LSC), la mayor entidad financiadora de asistencia legal civil del país. En California, eso habría significado la pérdida anual de $55.7 millones de dólares en fondos de la LSC, los cuales financian servicios para más de 165 mil personas en todo el estado, casi la mitad de las cuales (48 %) tuvieron casos relacionados con la vivienda.
Junto con otras propuestas federales, California corría el riesgo de perder un total de $187 millones en financiamiento para servicios legales. Si bien el presupuesto federal final incluyó una reducción menor, el financiamiento sigue siendo incierto, ya que debe volver a aprobarse anualmente. Además, las amenazas derivadas de la H.R.1 (2025) y de otras medidas federales aumentarán las dificultades para los californianos, haciendo que sea mucho más difícil costear el alquiler y otras necesidades básicas. Estas presiones ocurren al mismo tiempo que también disminuyen los fondos estatales y federales para la carencia de hogar, multiplicando la inseguridad de vivienda y estresando aún más los limitados sistemas de apoyo legal y de vivienda.
Mirando hacia al futuro, los responsables de formular políticas públicas pueden tomar medidas para proteger a los inquilinos de los desalojos
California aún no ha asumido un compromiso estatal de brindar apoyo legal a los inquilinos que enfrentan un desalojo. Los responsables de formular políticas cuentan con las herramientas necesarias para cambiar esta situación, comenzando con las siguientes medidas:
Establecer un derecho estatal a contar con representación legal para los inquilinos de ingresos bajos y moderados que enfrentan un desalojo y aumentar el financiamiento destinado a la defensa legal contra desalojos. Las inversiones estatales actuales en defensa legal contra desalojos son insuficientes en relación con la magnitud de la necesidad. Garantizar representación legal plena para todos los inquilinos que enfrentan procesos de desalojo, junto con sólidos esfuerzos de divulgación, educación y recursos, resulta mucho más rentable y eficaz que afrontar las consecuencias posteriores de la carencia de vivienda. The Roadmap Home estimó que el costo de proporcionar representación legal plena a una familia que se enfrenta a un desalojo formal es $3,500. Las investigaciones también demuestran que cada dólar invertido en asistencia legal produce una ganancia económica de por lo menos $7 dólares, pues reduce la presión en los tribunales, los sistemas de salud y los programas de redes de seguridad social.
Fortalecer y hacer permanente la Ley de Protección de Inquilinos (Tenant Protection Act, TPA). La TPA ha reducido los desalojos injustificados en los lugares donde se aplica, pero necesita ser más sólida y amplia. Los líderes estatales deberían hacer permanente la TPA, reducir el límite anual permitido para los aumentos de renta, eliminar exenciones para ampliar la cobertura a más inquilinos, incrementar los requisitos de asistencia para la reubicación y eliminar las remodelaciones sustanciales y las demoliciones como justificaciones permitidas para desalojar a los inquilinos por causas ajenas a ellos. La extensión de estas protecciones podría cubrir a 1.65 millones de inquilinos más.
Exigir la recopilación estatal de datos sobre desalojos y la publicación pública de dicha información. California no puede resolver un problema que se niega a medir ni calcular adecuadamente los recursos necesarios para subsanar. El estado debería exigir que los 58 condados recopilen y publican de manera uniforme datos sobre los resultados de los desalojos, incluidos los resultados de los casos, información demográfica y tasas de representación legal.
Establecer una ley estatal de subsanación del incumplimiento de pago de la renta. Siguiendo el ejemplo de 21 estados más, California debería permitir que los inquilinos que enfrentan un desalojo por falta de pago subsanen el incumplimiento de su alquiler —y permanezcan en su vivienda— mediante el pago del alquiler adeudado, incluso después de que se haya presentado una demanda de desalojo.
Destinar recursos de asistencia para la renta. Asignar recursos de asistencia con el pago de renta, incluidos subsidios de emergencia y subsidios parciales para el alquiler, vales de vivienda e iniciativas de realojamiento rápido, a fin de garantizar que las personas puedan permanecer en sus hogares durante períodos de crisis económica.
Conclusión
Mantener a los inquilinos de California en sus hogares mediante protecciones significativas para los inquilinos,apoyo legal robusto y políticas centradas en la equidad es una de las herramientas más eficaces que tienen los líderes estatales para proteger a los inquilinos de los desalojos. Esto es especialmente importante ahora, cuando los recortes federales derivados de la H.R. 1 y otras medidas regresivas amenazan con agravar los ya graves problemas de asequibilidad.
Fortalecer la base de ingresos públicos de California garantizando que las corporaciones más rentables y los californianos más acaudalados paguen lo que les corresponde podría generar los recursos necesarios para proteger a las comunidades. Al hacerlo, los líderes estatales contarían con los recursos necesarios para proteger a las comunidades de los perjuicios derivados de las medidas federales y financiar las protecciones para los inquilinos, la asistencia para el pago del alquiler y el apoyo legal que permiten que los inquilinos permanezcan establemente alojados en sus viviendas.
Salena Copeland y Lorin Kline de la Legal Aid Association of California contribuyeron a esta publicación.